News – Curated by Amanda Scott, Alias Group Creative
Follow her on Bluesky

Could Vitamin C Be the Secret to Keeping Your Brain Younger?
Lower vitamin C levels were linked to reduced brain volume and weaker neural connectivity in older adults, suggesting a potential connection between nutrition and brain health. Could a common vitamin help preserve the brain [...]
This Deadly Disease Was Wiping Out Humans 5,500 Years Ago
A new study suggests plague was already a deadly threat 5,500 years ago, striking small hunter-gatherer communities long before cities and agriculture emerged. For centuries, plague has been remembered as the disease that devastated [...]
China closing in but US leads in biotech quality, commercial reach, survey finds
SAN DIEGO, June 22 (Reuters) - China, which now conducts more clinical drug trials, opens new tab than the U.S., still lags in the quality and commercial reach of its biomedical science, according to a recent survey, opens new [...]

New method generates renewable supply of progenitor immune cells
In a paper published in Cell, a USC Stem Cell-led team reports a new way of generating a renewable and expandable supply of the progenitor cells that give rise to macrophages. These immune cells help [...]
Scientists Just Discovered a Cellular Survival System That Was Never Supposed To Exist
A surprising backup pathway allows cells to make a crucial amino acid when their primary machinery fails. For decades, biologists believed cells had only one way to access a molecule they cannot live without. New [...]
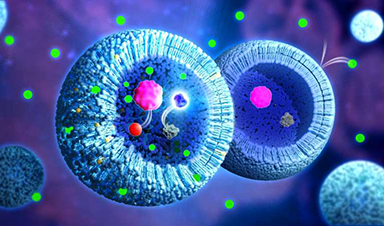
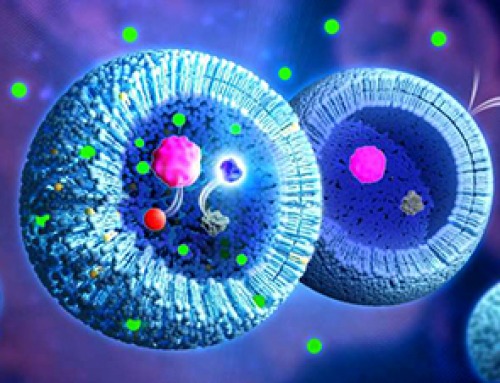
Artificial cells gain porous membranes, enabling lab reactions and drug release
Artificial cells created in the laboratory offer a wide range of potential applications. Until now, however, their membranes—unlike those of real cells—have been virtually impermeable. Researchers at the Max Planck Institute for Polymer Research, [...]

Popular Weight-Loss Drugs Like Ozempic Linked to Lower Breast Cancer Risk
Ozempic and similar weight-loss drugs were linked to a striking 30% reduction in breast cancer risk in a study of more than 110,000 women. Popular weight-loss and diabetes medications such as Ozempic, Wegovy, Mounjaro, [...]

Stanford Scientists Discover Explosive New Type of Immune Cell
Scientists studying the remarkable regenerative abilities of planarian flatworms have uncovered a previously unknown type of immune cell with an unusually destructive defense strategy. What if an immune cell could wipe out nearby threats [...]

Big Pharma-backed SonoThera sounds off with $125M series B for bubble-based genetic delivery
Bay Area biotech SonoThera is bubbling to a clinical boil after raising a $125 million series B with the backing of some of the biggest names in pharma. Vida Ventures led the raise, with the venture [...]

Joint initiative of 5 EU countries calls for ‘unified approach’ to pharma framework amid US drug pricing pressure
With drug pricing pressure building from the U.S., a healthcare-focused consortium of five European countries is calling for a “unified approach” to strengthen Europe’s pharmaceutical framework and access to innovative medicines. Belgium, the Netherlands, [...]
Our books now available worldwide!
Online Sellers other than Amazon, Routledge, and IOPP Indigo Global Health Care Equivalency in the Age of Nanotechnology, Nanomedicine and Artifcial Intelligence Global Health Care Equivalency In The Age Of Nanotechnology, Nanomedicine And Artificial [...]

Molecular Manufacturing: The Future of Nanomedicine – New book from NanoappsMedical Inc.
This book explores the revolutionary potential of atomically precise manufacturing technologies to transform global healthcare, as well as practically every other sector across society. This forward-thinking volume examines how envisaged Factory@Home systems might enable the cost-effective [...]
NanoMedical Brain/Cloud Interface – Explorations and Implications. A new book from Frank Boehm
New book from Frank Boehm, NanoappsMedical Inc Founder: This book explores the future hypothetical possibility that the cerebral cortex of the human brain might be seamlessly, safely, and securely connected with the Cloud via [...]
New book from Nanoappsmedical Inc. – Global Health Care Equivalency
A new book by Frank Boehm, NanoappsMedical Inc. Founder. This groundbreaking volume explores the vision of a Global Health Care Equivalency (GHCE) system powered by artificial intelligence and quantum computing technologies, operating on secure [...]
UCLA Scientists Uncover a “Hidden Weakness” in Some of the World’s Deadliest Cancers
A new study has uncovered an unexpected vulnerability in some of the deadliest cancers. Researchers at UCLA have identified a previously hidden weakness in some of the most aggressive cancers, pointing to a possible new way [...]
AI-designed universal coronavirus vaccine clears first human trial
Key Takeaways Super-Antigen Technology: Uses AI and machine learning to analyze viral genomes, creating a single vaccine that targets essential features across entire virus families, including coronaviruses and Ebola. Human Trials & Safety: Phase [...]