The current Bundibugyo Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda is exposing dangerous gaps in global health security. Experts warn that, amid the aid cuts and ongoing conflict in the region, the outbreak could become one of the deadliest Ebola epidemics to date. In the absence of an approved vaccine, the main tools for control are trust, community collaboration, and systemic empathy.
Systemic empathy describes how health systems care for people, including their own staff. It prevents stigma, which can catalyse a vicious cycle of contagion. In a stigmatised environment, symptomatic people and their families often avoid medical care out of fear of discrimination, forced isolation, and the denial of proper burial rites. At community level, the abrupt enforcement of coercive or heavily militarised measures intensify stigma, fuel rumours, and undermine cooperation.
The arson of an Ebola treatment centre in Rwampara, DRC, on 21 May 2026 is an example of how rapidly mistrust can destabilise response efforts. By contrast, keeping people informed about the risks of Ebola infection and adopting community centred approaches in the outbreak response improve trust and enhance participation in prevention and healthcare.
Collective government and community support for frontline health workers is equally important. In previous Ebola outbreaks, as well as the covid-19 pandemic, frontline workers were let down by instances of delayed or inadequate supply of personal protective equipment, failure to protect them from hostility, and unfulfilled promises of financial and emotional support. Frontline workers are the only defence between populations and the virus. A rift in frontline workers’ motivation can start a chain reaction of mistrust and stigma, disrupting the entire response.
With communities, it is vital to show that Ebola protocols are protective, not punitive. Steps can be taken to reduce tensions while preserving infection prevention and control standards. For example, building community care centres for patients awaiting test results—where families can monitor their loved ones from a safe distance—increases the likelihood that families will consent to patient isolation in specialised Ebola treatment units. Maintaining communication between patients in isolation and family through digital technologies and regular updates can further reduce the fear associated with treatment centres.
Safe and dignified burial involves informing the families at each step. Respecting religious practices, engaging families in customary prayers after the burial, and ensuring infection prevention throughout the process has proven more sustainable than rigid models that exclude families. If the deceased is a female, a trained female staff or family member should prepare the body for burial using full protective equipment.
Community engagement in outbreak settings should extend beyond traditional leadership structures to include women and young people, who are often central to caregiving and community mobilisation but remain excluded from decision making processes. The Rwampara incident is a stark example of the consequences of disengagement. The man who died was a popular footballer whose mother believed he had typhoid fever, and the crowd, upset by his death, reportedly believed the virus was a hoax.
To support frontline workers, it is critical that government and partner organisations are seen to fulfil their commitments rather than making empty promises. Health workers are already operating under extreme psychological and physical stress arising from exposure risk, shortages of protective equipment, insecurity, community hostility, and the deaths of colleagues. Government and health agencies must prioritise adequate protective equipment, psychosocial support, security arrangements, fair financial compensation, and meaningful community partnership through outreach activities.
Support and protection of frontline workers is especially important in areas such as Ituri province, DRC, where sustained conflict and insecurity complicate the outbreak operations.9 This needs to be balanced, since excessive militarisation of Ebola responses may itself erode public trust by creating perceptions that health operations are aligned with political or armed actors. Community-supported and locally negotiated protection mechanisms—such as engaging local volunteers in providing security to health workers moving to and from their health post—may be more effective than overt displays of force.3
In the absence of a licenced vaccine specifically for Bundibugyo Ebola, a community and its healthcare workers must be approached with systemic empathy. This is the core of outbreak response.
Footnotes
Competing interests: ZH is adviser to Gavi, the Vaccine Alliance (Eastern Mediterranean Constituency). He led Johns Hopkins University’s Health and Risk Communication Programmes in 2005-09 and 2014-18, and chaired Pakistan’s national task force on risk communication during the covid-19 pandemic.
AI statement: During the preparation of this work, the author used ChatGPT 5.2 (OpenAI) to improve spelling and ensure consistency in British English usage. After using this tool, the author reviewed and edited the content as needed and takes full responsibility for the content of the published article.
Provenance: Not commissioned, not externally peer reviewed.
News – Curated by Amanda Scott, Alias Group Creative
Follow her on Bluesky
Ebola control is weakened by mistrust and cultural insensitivity
Effective response depends on cooperation with communities and frontline workers, writes Zaeem ul Haq The current Bundibugyo Ebola outbreak in the Democratic Republic of the Congo (DRC) and Uganda is exposing dangerous gaps in [...]
Building the Brain Requires Millions of Dangerous DNA Breaks
Scientists discovered that building a healthy brain involves an unexpected step: young neurons routinely break and rapidly repair their own DNA. As the brain develops, newly formed nerve cells must travel through tightly packed tissue [...]

One Tiny Change May Explain How Viruses Jump From Bats to Humans
Scientists found that one tiny genetic change may determine whether a bat virus stays in bats or becomes a human threat. Most infectious disease outbreaks begin when a virus or other pathogen crosses from animals into [...]

Scientists Discover 250+ Genes That Could Lead to New Ways To Prevent Melanoma
The world’s largest study of mole genetics identified hundreds of genes tied to melanoma risk, uncovering potential new drug targets and paving the way for more accurate melanoma screening and prevention. Researchers at QIMR [...]
Breakthrough Diabetes Treatment Reprograms the Immune System
An engineered stem cell therapy reversed new-onset Type 1 diabetes in mice by shifting the immune system away from attacking insulin-producing cells. For more than a century, people with Type 1 diabetes have relied [...]

Taking the world’s temperature: WHO chief spotlights global health emergencies
Taking the world’s temperature on pressing health matters, WHO Director-General Tedros Adhanom Ghebreyesus provided the latest on current global challenges - and successes when it comes to international cooperation. “The outbreaks of hantavirus, Ebola and Marburg all show [...]
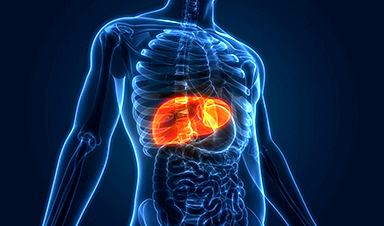
Scientists Create Tiny “Mini Livers” That Could One Day Replace Liver Transplants
Engineered tissue grafts could help perform key liver functions and benefit thousands of people living with liver failure. The liver is one of the body’s hardest-working organs, carrying out hundreds of vital jobs, from [...]
NanoMedical Brain/Cloud Interface – Explorations and Implications. A new book from Frank Boehm
New book from Frank Boehm, NanoappsMedical Inc Founder: This book explores the future hypothetical possibility that the cerebral cortex of the human brain might be seamlessly, safely, and securely connected with the Cloud via [...]
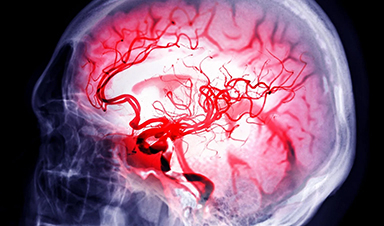
Scientists Discover Surprising Way To Help the Brain Recover After Stroke
A new study suggests that strengthening the body’s natural circadian rhythms may help the brain recover after stroke, even when treatment begins days after the injury. Every year, millions of people survive a stroke, [...]
Our books now available worldwide!
Online Sellers other than Amazon, Routledge, and IOPP Indigo Global Health Care Equivalency in the Age of Nanotechnology, Nanomedicine and Artifcial Intelligence Global Health Care Equivalency In The Age Of Nanotechnology, Nanomedicine And Artificial [...]

Younger Generations Are Aging Faster – and It May Be Fueling a Surge in Cancer
Younger generations may be aging biologically faster than those before them, and that shift could help explain rising rates of cancer at younger ages. For decades, cancer was viewed largely as a disease of [...]
Using Cannabis Could Raise Your Stroke Risk by 37%, Massive Study Reveals
Large-scale evidence suggests cannabis, cocaine, and amphetamines may directly raise stroke risk, including in younger adults. As recreational drug use becomes increasingly common, researchers are uncovering evidence that its health consequences may extend far beyond [...]

Could Vitamin C Be the Secret to Keeping Your Brain Younger?
Lower vitamin C levels were linked to reduced brain volume and weaker neural connectivity in older adults, suggesting a potential connection between nutrition and brain health. Could a common vitamin help preserve the brain [...]
This Deadly Disease Was Wiping Out Humans 5,500 Years Ago
A new study suggests plague was already a deadly threat 5,500 years ago, striking small hunter-gatherer communities long before cities and agriculture emerged. For centuries, plague has been remembered as the disease that devastated [...]
China closing in but US leads in biotech quality, commercial reach, survey finds
SAN DIEGO, June 22 (Reuters) - China, which now conducts more clinical drug trials, opens new tab than the U.S., still lags in the quality and commercial reach of its biomedical science, according to a recent survey, opens new [...]

New method generates renewable supply of progenitor immune cells
In a paper published in Cell, a USC Stem Cell-led team reports a new way of generating a renewable and expandable supply of the progenitor cells that give rise to macrophages. These immune cells help [...]